



WHY DOES VIOLENCE HAPPEN?
We used to think that child abuse, teen sexual assault, intimate partner violence, and elder abuse (as examples), were unique types of interpersonal violence. We searched for answers for why each of these types of violence happened and what we could do to stop them from happening. What we have learned through more than thirty years of research is that all these forms of violence have common underpinnings including having adverse childhood experiences growing up such as child abuse, sexual abuse, emotional abuse, neglect, witnessing violence, having a parent incarcerated, having a family member addicted to alcohol or substances, having a parent with a serious mental illness and other things that make it more difficult for children to develop secure positive attachments to adults and have adults in their lives who will positively guide them in learning how to understand and control their thoughts, emotions and behavior.
About thirty percent of us are fortunate and grew up without experiencing adverse events in our childhood. However, about 2/3 of us have experienced one or more of these adverse events. Looking into this more closely, 25% of us have at least one exposure to adversity, and 11% had at least six; all while trying to learn to walk, learn to read, and learn how to relate to other people.
Adolescents indicate they have been exposed to many different forms of interpersonal violence over the course of the past year such as sibling assault, child abuse, bullying, sexual harassment, street violence and other forms of violence (Finkelhor et al., 2015). In looking at gun violence, 17% of youth have heard gunshots or saw someone shot in the past year and 59% said they had these experiences during their lifetimes. How much violence overall have adolescents experienced? Surveys indicate that 48.4% of them reported having more than one exposure to violence over the course of one year and 15.1% reported experiencing six or more exposures (Finkelhor, Turner, Shattuck, & Hamby, 2013).
Children exposed to violence have more problems in school, increased emotional and behavioral problems and more problems developing social relationships, and are more likely to become involved in early sexual behavior and alcohol and substance use (Borofsky et. al. 2013; Lovallo et al. 2019). Children and teens with repeated exposure to violence are more likely to have parents who have abused substances (Dube et al. 2003) and are more likely to spend time with peers who abuse substances (Connolly & Kavish, 2019). Those with the highest rates of adverse experiences were the most likely to have problematic or addictive use of alcohol and drugs as adults (Bellis et al. 2019; Hughes et al. 2017; Wiehn et al., 2018). Use of substances decreases everyone’s judgement and thus will be just one more risk that they will be victimized yet again as they may not recognize the warning signs of violence and may not know what to do when they do recognize they are in danger. Exposure to violence can also lead to children and adolescents victimizing others (Connolly and Kavish 2019). This can include assaults on siblings, bullying, sexual assault, delinquent and violent criminal behavior (Brumley et al. 2017).
Thus, one answer to “why did this violent event happen,” is that those who commit violent acts were exposed to violence during their childhood and/or adolescence. Please review the charts below to see the rates of adverse events in three cities in Pennsylvania.


Adverse Childhood Experiences (Expanding the Concept of Adversity). Downloaded September 24, 2021 from: https://txicfw.socialwork.utexas.edu/wp-content/uploads/2017/02/Philly-ACES-revised_2015-1.pdf
How do Adverse Events Start in Childhood?
People are not born to be violent. However, engaging in an act of aggression is not unusual or rare. National surveys find that 32% of us indicated doing at least one aggressive thing and 30% of us say we engaged in two or more acts of aggression before we reached age 18 (Klevens et al., 2012). Most of us don’t engage in serious acts of aggression. However, the more adverse experiences someone has in their childhood, the more likely they may either be victimized by violence again, be the victimizer of others or both (Hamby & Grych, 2013).
Adults in the family are responsible for ensuring a safe environment for everyone to develop adaptive skills. However, adults are often the cause of violence erupting in the family. One adult in the family might be the only one to use violent tactics; for example, an adult who uses violence and coercive control in their relationship with an adult partner. However, both adults in the relationship may use violent tactics against each other. Across the lifespan approximately 35.6% of women and 28.5% of men will report experiencing a violent assault from an intimate partner (Black et al., 2011).
Adults using violent tactics against each other may also use violence in child rearing, and children in the family may learn to use violent tactics against each other. Thus, while it is possible that violence is a one-time event in the family, it is more likely that several forms of violence occur in the family, possibly across all generations including children, parents, and grandparents. There may be one or more members of the family that want the violence to stop but they don't take action because they don’t realize violence has no place in family life, because they do not know how to intervene to end violence, or they are prevented from doing so by a more powerful, violent family member (Hamby & Grych, 2013, Miller-Graff et al., 2018).
An adult trying to leave an abusive partner or trying to prevent an abusive partner from harming someone else are in danger of injury or death (Reckdenwald & Parker, 2010). Legal statutes label partner abuse as battery despite some being more dangerous and showing more lethality than others. Overall, men use more dangerous tactics than women when violence erupts. Women are more likely to indicate they are afraid of their partners than men. When someone dies, 1 in 3 women are killed by their male partners while 1 in 20 men are killed by their female partners (Reckdenwald & Parker, 2010). Adults who abuse their partners are not all alike, the frequencies of their assaults, the types of assaults, and the intensity of the assaults can vary. The most dangerous have been labeled by Frieze (2005) as engaging in intimate terrorism.
What makes the dynamics of family violence, more complex than that of stranger initiated violence, is that the victim might love the perpetrator and thus want the violence to end but not want to be separated from the perpetrator: for example, the person who engages you in sex against your will may also be the person who taught you how to swim and takes care of you when you are sick. As another example, victims might be terrified of those who hurt them yet need them to provide housing and food. There is short and long-term harm to children whether they are the ones being physically hit or emotionally abused or are witnessing this happening to someone else in the family (Felitti & Anda, 2010).
It is not always an adult in the family who starts the violence. Sometimes it erupts from a child or adolescent, such as in a sibling assault, with a ten-year old attacking his eight-year- old brother. It is the parents’ or adult caregivers’ responses to this assault that sets the stage for whether this violence reoccurs or is replaced by adult support for the ten-year-old learning to control strong negative emotions and urges as well as for learning problem solving strategies that don’t involve aggression or violence.
The answer to the question, “how do adverse experiences start in families," is simple in the sense that it is most likely to start with a family member, not a stranger. However, it is complex in the sense that it can start with any family member and involve many different types of violence. Different types of violence often happen together. For example, a parent calling a child a loser (emotional abuse) while hitting them with a belt (physical abuse). There may only be one act of violence in a family. However, it is most likely that there are many times when the violence has erupted. Whoever commits an act of violence within the family, it is always the adults who are responsible for taking the necessary steps to ensure a safe environment.
Please review the charts below to see the rates of different forms of adverse events in three different cities in Pennsylvania.



Child Protective Services Annual Report (2019). Retrieved September 24, 2021 from: https://www.dhs.pa.gov/docs/Publications/Documents/2019%20child%20prev.pdf
Why are Different Forms of Violence Related to Each Other?
There are common risk factors for all forms of interpersonal violence including childhood exposure to adversities such as physical abuse, sexual abuse, neglect, emotional abuse, witnessing intimate partner violence, having a parent with a substance abuse problem and/or mental health problem, a parent in prison or involved in criminal activity, and parental divorce, exposure to racism and discrimination as examples. An accumulation of any of these types of adverse events can lead to toxic stress resulting in children and youth having delays in cognitive, emotional, social and behavioral development.
These delays can result in children and youth being more vulnerable to involvement in risk taking behavior such as alcohol and drug use, early engagement in sexual behavior and a lack of attention to academic skills and involvement in prosocial behavior. These children and youth are more likely to engage in social relationships within a deviant peer group as they withdraw from or are rejected by more prosocial peers. All of this makes it more likely that they will have further exposure to violence. In these violent episodes, they may either be the victims, the perpetrators, or across different types of violence sometimes be the victim and sometimes the perpetrator of violence (Brown et al., 2009; Felitti & Anda, 2010; Felitti et al. 1998; National Scientific Council on the Developing Child, 2014). It is the frequency of exposure, not the type of violence experienced that predicts future victimization or engaging in perpetration against others. Engaging in one type of perpetration leads to increased odds (1.5 to 4 times) of engaging in another form of perpetration (Klevens et al., 2012).
Thus, many types of violence can occur within the same people including as examples: the adult who physically assaults friends in a bar when drunk and abuses intimate partners when at home; a twelve-year-old who is physically abused by a parent, may assault younger siblings when “babysitting” and be a bully at school. A ten-year-old who was sexually abused by a parent may be submissive towards a bully at school, may as a teen be submissive towards dating violence and not be effective at stopping a partner from abusing their children when an adult.
Living with violent adults in the family or within a community where there is a great deal of violence provides role-models for violent behavior and the development of internalized norms that violence is acceptable within close relationships or to achieve status, or to solve problems. There are also cascading negative impacts to repeated exposure to violence. This type of toxic stress can literally change the architecture of the brain making it more difficult for children and adolescents to make adaptive decisions later on in life (Appleton et al. 2019; Bellis et al. 2018; Oh et al. 2018; Larkin et al. 2014; Manyema et al. 2018). We all have areas of our brains that are designed to help us take actions such as fleeing or fighting for the sake of our immediate survival. We also have areas of our brains that help us with impulse control, stopping and thinking, and review of the consequences of our actions for the sake of achieving long-term vs short-term goals.
The areas of the brain concerned with our immediate survival develop first. However, as we move through childhood and adolescence these areas come more and more under the influence of the areas of the brain that support our long-term well-being. However, toxic stress or chronic trauma from violence during childhood and adolescence can overload our “survival” system and impact our ability to regulate our thoughts, emotions, and behavior for the long term. With enough overstimulation, dysregulation of our stress system can occur. This leads to responses in the moment rather than responses that lead to longer term survival and well-being.
The overuse of our survival system, and/or dysregulation of our stress system can have a broad impact on our development, making it harder for us to learn from experience and more likely to experience emotional, social and cognitive delays in comparison to our peers (De Bellis, Woolley, & Hooper 2013; Gunnar & Quevedo, 2007; Lupien, McEwen, Gunnar, & Heim, 2009). Thus, toxic stress resulting in developmental delays may help explain why children and youth who have been repeatedly exposed to violence may literally have more difficulties learning from their experiences and thus continue to make the same bad decisions despite not likely the consequences they are getting.
How might toxic stress directly impact the behavior of children and adolescents? It can lead children to be either under (hypo) or over (hyper) responsive to signs of potential threat in the environment. Children who are hypo-aroused may not take steps to protect themselves in potentially dangerous situations. For example, Kevin, who has been beaten up on the playground after asking a bully if he can join a baseball game, might do the same thing the next day and get beaten up again.
How might Kevin behave if he was hyperresponsive to signs of threat? Children who are hyper-aroused may find neutral situations to be threatening and respond with flight or aggression. Thus, if a classmate stepped backward in line and accidentally stepped on Kevin’s foot, he might assume it was intentional and immediately punch this classmate. Children who are hyper-aroused may also spend so much time scanning the environment for signs of danger that their brains are less attuned to new aspects of the world they should be learning about. Thus, a hyper-aroused Kevin might be failing or underperforming in school because he doesn’t have the freedom to let his mind pay full attention to what a teacher is saying during class lessons. In efforts to remain safe, hyper-aroused Kevin might engage in verbally or physically aggressive behavior in class that leads him to spend time sitting outside the classroom or in the principal’s office; this again can lead to decreased academic achievement as he is being separated from classroom experiences where he could learn important skills (National Scientific Council on the Developing Child, 2014).
People may show numbing of their emotions after repeated exposure to violence. Numbing of fear responses was found to occur as a result of exposure to violence in a variety of settings whether they were the direct victim of the violence or witnessing it. Numbing of fear responses, can prevent children and youth from being able to weigh the risks of personal harm if they engage in high-risk behaviors (Horan, Allwood & Bell; 2011). Numbing of sadness has also been found to occur. In this type of numbing, children and youth may not feel sad when someone they care about is very ill or dies. This type of numbing has been found related to engaging in aggressive and delinquent behavior (Allwood et al., 2011).
The answer to why different forms of violence may be interconnected is that the same risk factors exist across most forms of violence and the same factors that support us learning not to be violent are also the same across most forms of violence.
Children Show Complex Responses to Adverse Events
Children respond in diverse ways to being exposed to violence. How might a particular child respond to adverse circumstances? It will be a complex blend of innate tendencies for responding to stress, the positive influences in their lives, past negative influences and so forth (National Child Traumatic Stress Network, 2012). Responses to adversity, violence, and trauma are complex. Children have been found to respond by blaming themselves, blaming others, or showing the world only their best behavior.
Children who blame themselves
Children can turn inwards and blame themselves for the bad things that happen and may feel anxious, depressed and/or withdraw from others. This may reduce the likelihood of them noticing any positive and supportive responses from others. If others actively reach out to these children, this can help them recover their emotional balance after exposure to adversity. Without enough help, these children can develop mental health problems such as anxiety and depression and experience prenatal and postpartum depression, as well as engage in self-harm or suicidal behavior (Mersky and Janczewski 2018; Slavich et al., 2019; Wiehn et al. 2018).
Children who blame others
Children can look outside themselves and look at others as causing their problems. These children may feel angry, frustrated, and wish to punish others. These children might go to school and throw a chair when frustrated, feel they must control what happens in the classroom to be safe, and/or engage in other behaviors that can make adults and children withdraw from contact with them. This acting up behavior can make it less likely that other children or adults will respond positively to these children, despite this being what they need. Instead of helping these children develop positive attachments, they may reject or punish these children. These reactions, while understandable, further reinforce the lessons they learned from adversity- that they are alone in dealing with it. These children may develop externalizing behavior, delinquent, and criminal behavior (van Duin et al. 2019).
Children who show the world their best behavior
There are some children who seem resilient in the face of adversity in their lives. They may work hard at home and in school- being adult pleasers who do whatever they can to earn praise (National Child Traumatic Stress Network, 2012). While these children and youth may earn good grades in school and achieve jobs that other people envy, the adversity in their past has left its marks and no one knows they need help to end episodic nightmares, fears of being alone, lack of trust in intimate relationships and other possible negative consequences of their past.
Commonalities Across Types of Reactions
While children show complex responses to their past experiences with adversity, there may be some common responses. For example, they may have more difficulty responding adaptively to their emotions, controlling how emotional they get, and learning from experiences that occur within highly emotional contexts. They are more likely to have disordered use of substances or substance abuse and higher rates of poor self-esteem, lower rates of global well-being, and more pessimistic views of their lives (Brumley et al. 2017; Cole et al., 2013; Weiler and Taussig 2019).
Please review the charts below to see the rates of different forms of dysfunctional behavior and violence in three different cities in Pennsylvania.
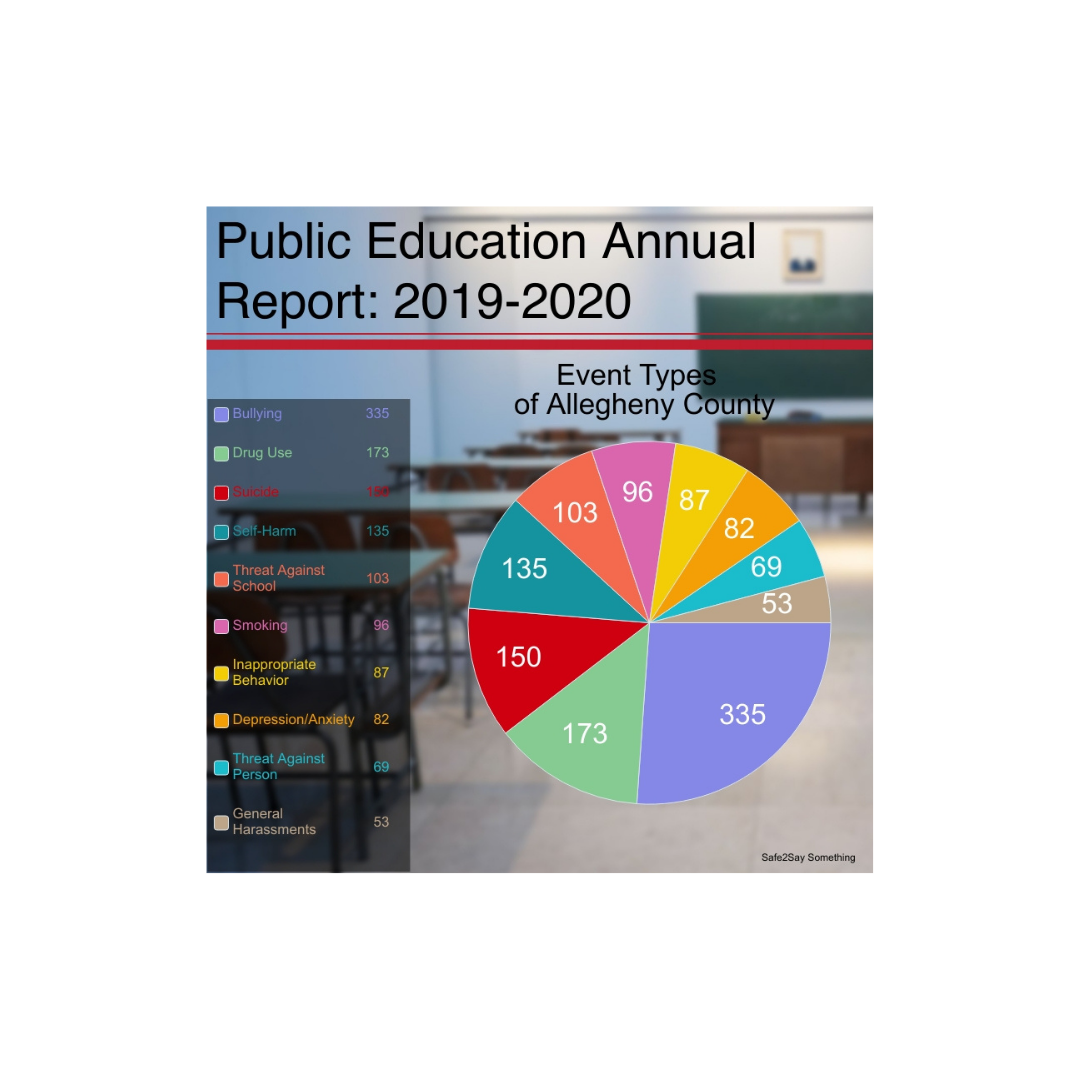

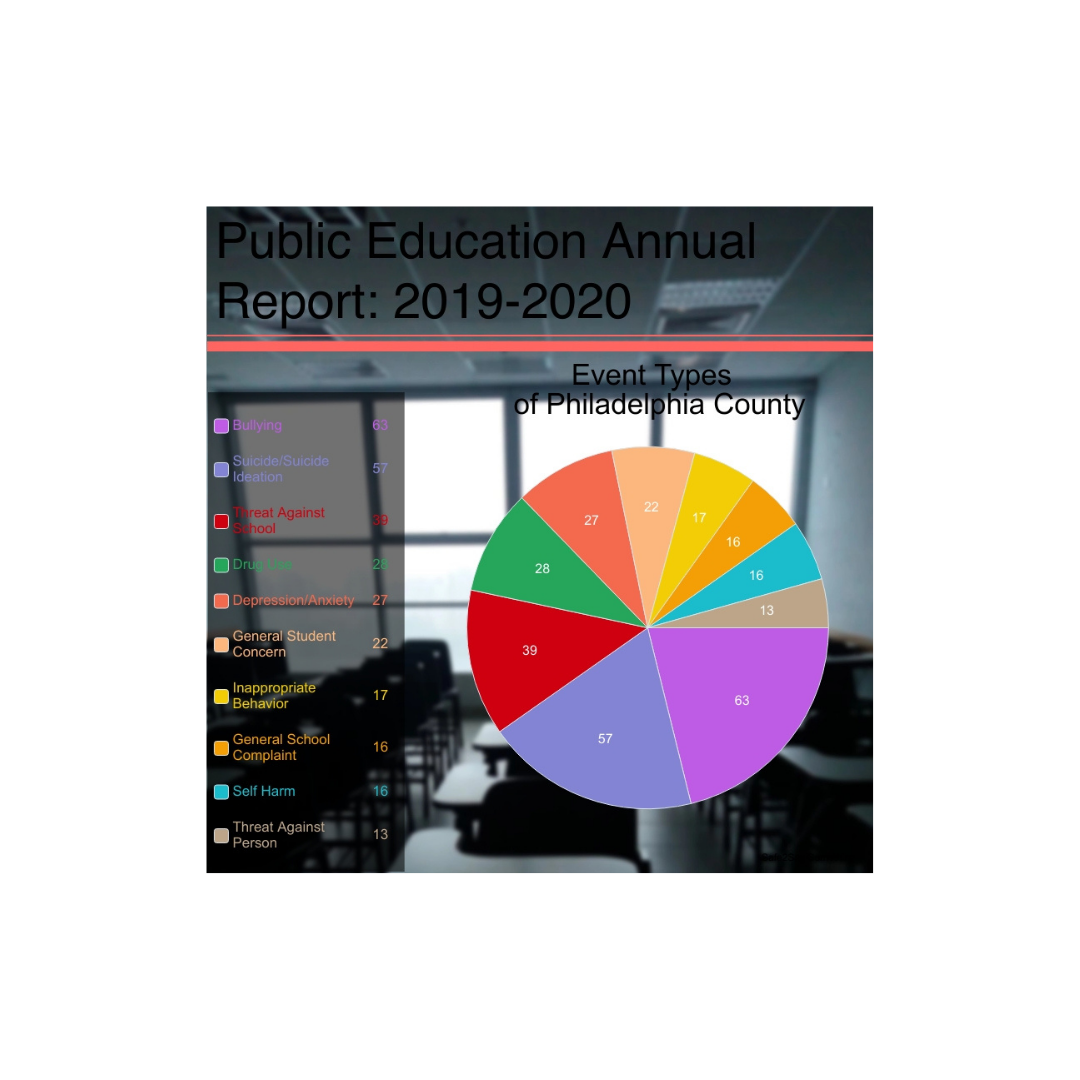
These charts were developed from: safe2Say Something Annual Report (2019-2020 School Year) Downloaded September 24, 2021 from: https://www.safe2saypa.org/wp-content/uploads/2021/01/2019-2020-S2SS-Annual-Report-FINAL.pdf
How does Violence Travel Across Generations?
About 1/3 of individuals who have been the victims of abuse and neglect by their parents do not go on to abuse and neglect their own children. However, it takes commitment to both “not wanting to be like their parents” as well as the effort needed to learn the skills needed to raise children adaptively. Adults need to help children and adolescents learn how to control their emotions, stop and think, as just a few of the skills that are critical to academic and employment success, as well as the ability to form and maintain stable and adaptive relationships with others.
It is both the exposure to violence as well as the other consequences of living in violent families that begins the cascading negative impacts that lead children and adolescents to follow the same path forward their parents took. The direct impact of exposure to violence includes being physically harmed by violent acts, observing violent acts, and being ignored when needing help. The indirect impacts include having parents who may be using alcohol or substances to enjoy life or to escape feelings of hopelessness and depression. Thus, rather than teaching their children how to deal with negative feelings and problems using adaptive mechanisms, they are role models for harmful strategies.
Living with violence can lead children to becoming numb to emotions or overreacting to them. This lack of appropriate emotional regulation can lead these children to be socially isolated or rejected by peers. It is also associated with similar difficulties controlling thoughts and behaviors. Taken together these factors are related to poor school performance and later difficulties with employment success and having stable adult relationships (Borofsky et al., 2013; Eisenberg et al., 2014; Sunirose, 2017).
Children learn social skills through interactions with others. Whether it is due to being overly aggressive and impulsive, or overly controlled and withdrawn, these children are not receiving the type of social feedback that will help them further develop the emotional, cognitive, and social skills needed to have strong and healthy interpersonal relationships. Research has shown that exposure to any form of violence increases the likelihood of being exposed to other forms of violence. Children who come to school already abused and/or neglected are at greater risk for: being a bully or being bullied; associating with deviant peers; being sexually or physically assaulted as they begin to date; becoming involved in intimate partner violence as adolescents; becoming involved in intimate partner violence within adult intimate relations; having poor child rearing skills and thus beginning to abuse or neglect their own children; and, continuing to experience violence even as older adults by their partners, their own adult children, or others (Acierno et al., 2010, Espelage et al., 2018; Foshee et al., 2016; Parker, Debnam et al., 2016; Wilkins et al., 2014; Vagi et al., 2015).
Thus, why someone might become a violent parent when they set out not to be is that they didn’t get the help and support they needed to learn adaptive parenting skills.
Social, and Political Supports for Interpersonal Violence
There are many social environments and political policies that can increase the likelihood of interpersonal violence occurring. Individuals at lower ends of the socioeconomic status continuum are exposed to environments where more violence occurs. Those who live in poverty within urban settings may be exposed to street violence, illegal drug use on the streets, neighbors who are more suspicious of the community, and less positive police support. Exposure to a violent event while on the way to school, walking to the store and so forth can make violent behavior seem more common or natural. Poor children often attend poorer quality schools where teachers may have less time and energy to help them engage in resilient behaviors that make violence less likely. For example, helping the child struggling in school to persist, set goals and achieve academically. Having academic success sets the stage for later success as an adult in the workplace (Masten, 2014).
Other sources of toxic stress from growing up in areas of concentrated poverty may include frequent food or housing insecurity, lack of adequate medical care, living in deteriorating neighborhoods that may be close to environmental hazards or exposure to community violence, illegal substances, and few opportunities for positive recreation or employment (Anderson, 2011; Sampson, 2012). In addition, exposure to racism and discrimination in the community has been found to be a significant form of adversity that can cause chronic stress in children and adolescents (Cronholm et al., 2015).
Institutional forms of oppression such as sexism and racism have been found to increase the sense of hopelessness in the future that fuels interpersonal community and other forms of violence. Institutional forms of oppression that lead to the school to prison pipeline further decrease the sense of hope in a future free of violence. For example, people of color who have been found to use any substances represent 13% of all drug users, yet they are almost half of those convicted of a crime related to drugs (Mauer, 2009). People of color are over- represented at every step of the criminal justice system and White individuals with higher incomes are much less likely to serve time for their offenses than people of color who commit similar offenses. In addition, drug policies have led to 20-fold increased incarceration of drug offenders- mostly people of color (Brucknor & Barber, 2016; Green, 2012; Schmitt, Warner, & Gupta, 2010). This leads to community wide loss of hope and increases in anger that can fuel interpersonal violence.
Raising children and adolescents is hard for everyone and contains many different types of challenges. Trying to do this, while having a less than optimal educational background, vocational, health, and income inequality, and food and housing insecurity makes raising children in a healthy and supportive manner extremely difficult. Adults exposed to adversity in childhood may start out as new parents trying not to be like their own parents - they have the will to be different. However, if they don’t have the needed education or income, they may lack the skills needed to make this wish a reality. Therefore, they may unintentionally continue to transmit violent or neglectful parenting practices to their own children.
Parents can take many different pathways that result in harm to their children. For example, a parent who fears losing control and abusing their children, may instead avoid setting any limits on their children’s behavior. Without any rules to guide themselves, these children may get into dangerous situations, be repeatedly injured, fail in school, get involved in sex and drugs in their early years and so forth; the fear of being abusive has led these parents to seriously neglect their children. On the other hand, parents may start out trying to be more patient with misbehavior than their own parents but hit roadblocks to doing this. Children repeatedly make the same mistakes prior to learning how to behave differently. In addition, they need to know “what to do”, not just “what not to do”. Thus, a parent who has repeatedly told a child to not take money left on the counter, can find the child still taking money over and over. Not recognizing the child needs help learning impulse control, the adult may come to the conclusion that the child’s behavior is a sign of serious immoral behavior that requires serious consequences; potentially leading to physical and emotional abuse. This type of mistaken conclusion comes from a lack of understanding of child development. There are many “normal problems” of development that can seem like serious problems to an unaware parent. For example, it is typical that two-year-old children will attempt to push boundaries and discover what they can and cannot do. It is typical that they will have temper tantrums when prevented from doing what they want. However, without a knowledge of child development, this behavior can be perceived as intentionally disrespectful to the parent and a sign of refusing to accept limits from the parent- which may trigger a loss of control (Hamby & Grych, 2013).
If parents who experienced violence in childhood want to escape the traps that lead to the intergenerational transmission of violence, we must reach out and provide comprehensive services to all members of an abusive and/or neglectful family. Each family member needs support to learn the skills that are necessary for adaptive living. These will include learning skills that reduce the risks of being involved in future acts of violence as well as the skills that support resilient functioning.
Should We Help Perpetrators of Violence?
Hearing about someone who abused, neglected, assaulted, raped, or neglected someone else might fill you with feelings of anger and thoughts of revenge. How could a parent intentionally starve a child to death? How could a teen beat his younger brother up? How could an adult rape or sexually assault someone in need of their care? What is your gut reaction to this person? Do you feel they should receive help?
When we look at the backgrounds of those who get harmed and those who do the harming, we find similar risk and protective factors. Risk factors include a lack of support in learning how to control emotions and behavior, exposure to family conflict including adults engaged in violent behavior towards family members and other factors that result in the growing person not developing safe and secure attachments to adults (Fowler & Dillow, 2011). When we don’t have secure attachments to adults, it leads to cascading emotional problems that could involve having a restricted range of emotions, being numbed to our emotions so we don’t recognize cues that we are in danger, or experiencing overarousal so we become aggressive to protect ourselves when in fact we aren’t in danger (De Bellis et al., 2013)
If we look at the symptoms of adults who get harmed and those who do the harming, we find they show similar problems. This can include problems such as anxiety, depression, post-traumatic stress disorder, antisocial personality disorder and borderline personality disorder (Spencer et al., 2019).
People who engage in violence can change. As they were developing, there were times where interventions could have taken them off the path of engaging in violence to solve their problems. It might be easier to see how different forms of help could make a significant difference, if we examine a hypothetical case. Let’s assume that 35-year-old adult, White male Jeff has been found guilty of sexually assaulting a cognitively impaired person who he was paid to take care of. What is your gut reaction to Jeff? What you think should happen to him?
Now, let’s go back in time to when he was 14. Jeff is socially isolated in High School. The only other peers who interact with Jeff are the other troubled teens at school. He has not started dating yet, but he and his male peers have begun sharing aggressive sexual fantasies with each other and may enjoy playing video games that include sexual violence or watching movies that involve men sexually controlling others. They don’t understand how to engage in the type of relaxed, social exchanges that build positive relationships with possible dating partners. Jeff and these other teens are at high risk for acting out their aggressive sexual fantasies if things continue as they are.
Today, Jeff has come to school after receiving abusive discipline from his father who also has emotionally berated him to start acting like a “real man”. Jeff's gym teacher, who hasn’t paid much attention to him in the past, notices pain across Jeff's face when a teammate touches his shoulder during a basketball game. The gym teacher approaches Jeff and tries to ask him about this, but Jeff just tries to walk away. Not put off by this, the gym teacher sends Jeff to the nurse who discovers huge welts from a belt scoring Jeff's back. What is your gut reaction to Jeff? What you think should happen to him?
The nurse is a mandated reporter of suspicions of child abuse and calls Child Protective Services. Assume that a well-trained interviewer talks to Jeff about the welts on his back. Jeff has now had three contacts with adults who appear to be showing concern for his welfare. He tried to just throw the coach’s concern away, but he was sent to the nurse anyway. Jeff tried to show how tough he was to the young, attractive nurse at school, by showing his back. While praising his courage, the nurse said Jeff deserved help and called in more help. A well-trained Child Protective Services worker gained even more traction with Jeff, who then began telling him about the regular physical and emotional abuse he received at the hands of his father. He also indicated that despite asking for help from his mother when he was younger, he has given up asking for this. It only seemed to make her dive deeper into alcohol abuse and turn her back on his situation. What is your gut reaction to Jeff? What you think should happen to him?
Jeff’s behavior as an adult has been to sexually assault an impaired adult who needed his help; this is totally unacceptable. However, he has not engaged in the most extreme forms of abuse of others seen by Child or Adult Protective Services. Approximately 1-2% of children evaluated for child maltreatment meet criteria for being tortured (Knox et al. 2014a). Children who are tortured may have been denied food or water, not allowed to use toilet facilities, bound or restrained, locked in small spaces, forced to eat excrement and so forth.
Perpetrators of child torture are not like those who episodically lose control and physically harm a child or dependent adult because they don’t know what to do. The perpetrator of torture engages in a program of psychological and physical assault including intense humiliation and terror. The acts are intended to cause serious harm and/or death; the victims are often programmed to believe the torture is their own fault. The perpetrator does not seek out any medical help for the victim however severe the physical injuries; the victims may die without intervention (Allasio & Fischer 1998; Knox et al., 2014 a). Behavior of the perpetrator may get worse and worse over time (Turner et al. 2010). It is important to do careful investigations to make sure that cases of child torture are not misidentified as child abuse as the child’s live is literally in danger if left with the torturer. It is not safe to send a child back home to someone who tortured them, and the torturer is not safe left out in the community, despite their current victim having been removed from the home (Ratnayake Macy, 2020).
If we want to end interpersonal violence, then the answer to, “should we help the perpetrators of violence,” is clearly yes. However, the level of risk a perpetrator represents to others, needs to be taken into account as to whether they can receive services and remain in the community, or if they need to be within a contained environment such as a jail or prison while they receive opportunities to learn how to live without violence.
The charts below show just how common it is for incarcerated men (N=3,895) to have experienced trauma in their childhoods, as adults, and both as children and as adults:

Wolff, N., & Shi, J. (2012). Childhood and adult trauma experiences of incarcerated persons and their relationship to adult behavioral health problems and treatment. International Journal of Environmental Research and Public Health, 9, 1908-1926; doi: 10.3390/ijerph9051908
Factors that Support Resilience
Children and adolescence are not always traumatized or harmed in the long run by adverse experiences. Healthy development requires what Masten (2004) called ordinary magic. This includes an environment in which there are adults who helped them learn to: form positive emotional bonds with others; control their thoughts, feelings, and behaviors; succeed in school; develop a belief that they can succeed and achieve even when things are very hard; and develop faith or hope that life has meaning and that a positive future is possible. An important way we can help children and adolescents recover from adverse circumstances is to increase and support these forms of ordinary magic. Achieving at school is a struggle for students who are raised within poor communities where parents may work very long hours to keep their families housed and fed. In addition, schools are provided funding by property taxes. This leaves poor communities with poorly funded schools. When programs are funded in poor communities that help children develop school readiness skills, it has been found to reduce later problems with the criminal justice system by 75 % (Heckman, 2013). Ending institutional racism, sexism, and other forms of oppression through accurate history education in schools, dismantling judicial practices that have made prisons into warehouses, and political practices that serve to maintain disadvantage can help to renew hope and optimism within communities and support resilience.
How might you answer the question, “how will Kayla respond to exposure to violence”? The unsatisfactory answer is, “it depends.” This is because everyone has a complex blend of innate tendencies for responding to stress. In addition, recovery from exposure to violence requires support for understanding what has happened and how to build a positive future. Thus, the more factors supporting resilience Kayla has in her life, the more likely she will behave adaptively following an exposure to violence.
TO LEARN ABOUT EFFECTIVE HELPING STRATEGIES click here
TO LEARN ABOUT PREVENTING VIOLENCE click here
This is funded with PA Tax dollars. The opinions, findings and conclusions expressed within this publication are those of the author(s) and do not necessarily reflect the views of PCCD.